Today, psychology and psychiatry are becoming more and more popular. On one hand, this allows for information, accessible explanations, and awareness-raising. On the other hand, it sometimes leads to misconceptions about different terms and expensive diagnostic requests for individuals, both psychologically and financially.
Today, it seems that more and more people feel different, out of sync with a certain social or media norm. It is then legitimate to seek an answer in a diagnosis, a label that can characterize us and make sense of this painful feeling of difference.
If the feeling of being out of sync can, for some, correspond to an atypical way of functioning, this is not always the case.
I wanted to clarify some of the popular “psy” terms here. I understand that I may be entering into a debated and sometimes contentious subject, but it is important for me to bring some clarity, at least based on my experience as a psychologist.
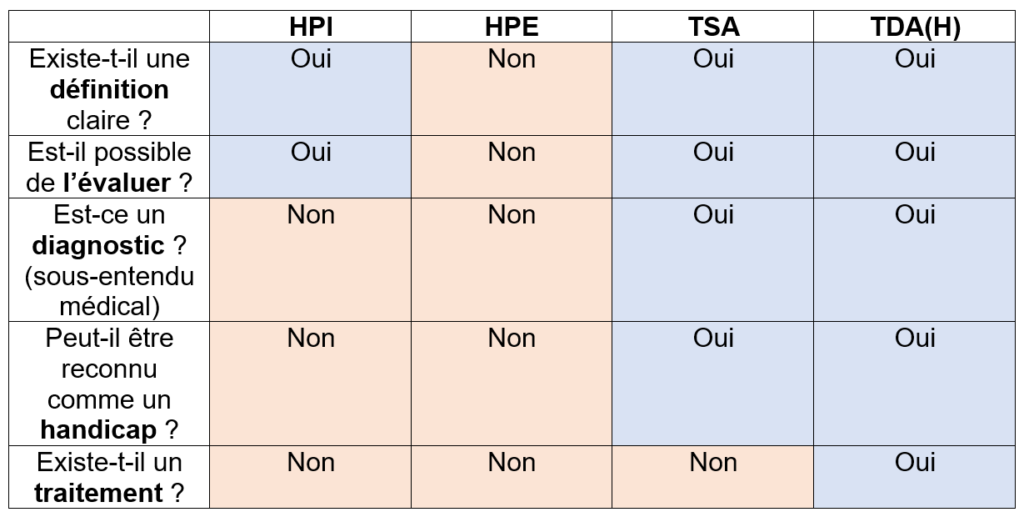
The HPI: Diagnostic or Not Diagnostic?
High Intellectual Potential corresponds to an identification through an IQ test. It is not a medical diagnosis and is not considered a disability.
Traditionally, in psychology, we define intelligence as an ability to adapt (which we then use or not, depending on other factors such as life history, temperament, possible cognitive particularities, etc.). Psychologists have looked for intellectual abilities that allow us to adapt. From there, the IQ test was created. It is a statistical test that is regularly re-edited. To construct it, a representative sample of the population is solicited for each age group. The performance of these individuals is then distributed according to a Gaussian curve (= bell-shaped curve). Then, the performance on each exercise (and in each domain) of each person who takes the test is compared to the performance of people in their age group. In summary, we place the person’s performance on the bell curve. The definition of HPI is: total IQ above 130, which corresponds to 2.2% of the population. In France (which is not necessarily the case in some other countries), some professionals associate HPI with personality characteristics. Identification is sometimes based on personality style. This is a psychological interpretation that, in my opinion, must be taken with great caution and can lead to biases in self-representation. Only the IQ test can validate HPI.
And what about “zebras” in all of this? HPI has received several names: giftedness, precocity, HP, HPI, HQI, and zebras. All these names, in my view, refer to the same thing, the same concept. I usually use HQI (a literal translation of what we are trying to convey: High Intellectual Quotient) or, preferably, HPI because it seems to me to be the terminology that is closest to the factual: a measurable intellectual potential that will then be used or not. Sometimes, we simply refer to it as HP. The term “giftedness” seems connoted (although I use it occasionally) and the term “precocity” is not very significant for adults. As for the term “zebra,” it seems associated with “psy” representations that I do not share… and besides, although we are also animals as humans, our cognition is not quite the same 😉
The HPE: Diagnostic or Not Diagnostic?
High Emotional Potential is a notion that is increasingly talked about. To my knowledge, it is a notion that is not yet defined scientifically and does not have consensus among psychology professionals. Therefore, there is no, to my knowledge, valid test to reliably assess it.
Sometimes, it is assessed in a “clinical” way, that is, based on the psychologist’s interpretation or representation. There is therefore a subjective aspect to it. Sometimes, it is assessed using tests designed to measure something else. For example, I have seen the use of the EQ questionnaire (= empathy quotient) in this sense. However, this questionnaire was designed and validated for screening for autistic disorders. The EQ questionnaire has a threshold that allows for the evaluation of when there are difficulties in empathy that may require further assessment to explore the possibility of autism. It was not created and validated to measure HPE. To make a metaphor, it’s a bit like trying to measure body temperature with a thermometer that has a temperature range from 0 to 30 degrees and deciding that 25 degrees corresponds to a normal body temperature.
It is entirely possible that HPE does exist: many human characteristics can be distributed on a bell curve, just like HPI. However, in order to assess it, there must first be agreement on its definition and a reliable and valid tool to measure it. The answers will come from scientific research in psychology.
The TSA: Diagnostic or Not Diagnostic?
Autism Spectrum Disorder is a medical diagnosis listed in a medical directory such as the DSM-V. It is considered a Neurodevelopmental Disorder (TND). Only a doctor, usually a (child) psychiatrist, is authorized to make the diagnosis based on multidisciplinary assessments. TSA can be recognized as a disability, so it is possible to submit an application to the MDPH (Maison Départementale pour les Personnes en situation de Handicap) to have the environment adapted to provide individuals with ASD with the same opportunities as others to build their lives.
One can feel different and not have ASD, and one can feel different and have ASD. ASD encompasses several characteristics of social communication, behavior/interests, and sensory issues. There are generally three steps to diagnosis:
- Identification: by the person themselves, parents, healthcare professionals, or teachers.
- Screening: using questionnaires and scales, sometimes available online, which are not sufficient to make a diagnosis.
- Diagnosis: which initially requires a specialized medical consultation, followed by often multidisciplinary assessments that assist the doctor in the diagnostic process.
People with ASD require specific psychological support to help them decode our social world. Predictability, structure, and clarity in the environment, including the social environment, are essential. It is also necessary to use sensory accommodations.
It should be noted that diagnosing ASD in adulthood can be very difficult. On one hand, the person may have developed psychological difficulties (often anxiety and depression) that complicate the diagnostic process. On the other hand, the person may have also developed adaptation and coping strategies that provide them with tools to adapt and mitigate the expression of autistic characteristics, which also complicates the diagnostic process.
The TDA(H): Diagnostic or Not Diagnostic?
Attention Deficit Hyperactivity Disorder is a medical diagnosis listed in the DSM-V. It is considered a Neurodevelopmental Disorder (TND). Only a doctor, usually a (child) psychiatrist, is authorized to make the diagnosis. TDA(H) can be recognized as a disability by the MDPH, meaning that the environment must be adapted to provide individuals with the same opportunities as others to build their lives.
The diagnosis is made by a doctor, preferably (but not always) based on a neuropsychological assessment, which may include an IQ test, an attention assessment, and assessments of memory and executive functions (organization, planning, impulsivity, etc.). It should be noted that neuropsychologists are psychologists who have specialized in neuropsychology during their training. As for me, I am a clinical psychologist, which is different. I received specialized training in psychotherapy and psychopathology.
For children, there is a treatment with psychostimulants, which is sometimes also prescribed for adults. The brains of people with TDA(H) need stimulation. Once sufficient stimulation is provided, agitation and impulsivity diminish, concentration improves, and emotional regulation improves. There are also specific interventions, such as cognitive remediation by neuropsychologists or emotional-cognitive-behavioral therapies by trained psychologists. Like ASD, but specific to TDA(H), the environment can be adapted to limit distractibility and impulsivity.
It should be noted that diagnosing TDA(H) in adulthood can be difficult for the same reasons as those mentioned for ASD.
Other Diagnoses and Non-Diagnoses
While these terms are the most well-known, others remain much more discreet in our media, such as Social Communication Disorder or Developmental Coordination Disorder, which are also TNDs listed in the DSM-V. And let’s not forget about difficulties that have become part of everyday language but may still be unknown (such as dyslexia, for example). Some individuals are also affected by psychological suffering (such as anxiety, depression, etc.) and/or trauma related to their life history or family transmission, and/or difficulties in personality structuring. It is worth noting that there are different types of personalities, and it seems to me that none of them perfectly align with the social norm to which many of us seem to relate less and less.
In conclusion, humans are of great complexity and richness… and that is a blessing!
And let’s not forget what is, in my view, the most important thing: each of us, regardless of our personality, diagnosis, or non-diagnosis, has resources, strengths, and vital impulses from which to draw to overcome suffering and difficulty, with the support of a professional when needed. It seems to me that the most enriching therapeutic journey is the one that leads us to know ourselves, our own functioning, our needs and limits, and the way we need to encounter others and the world—more or less. This self-knowledge can be realized without value judgment, without comparison to social norms. We can discover it through reflection, experience, joys, and sorrows… This self-knowledge allows us to make life choices that are ours, respecting others, choices that have the potential to help us flourish a little more each day… Towards a sense of autonomy and the wonderful feeling of being alive.